
Blog
Heads are spinning and people are asking why

This week I want to address a specific variant of a condition that I’ve been seeing a lot of lately – dizziness. Primary Care doctors in the U.S. see about six million patients a year who complain of “dizziness.”
Dizziness means different things to different people and can be a symptom of many different medical conditions. People use “dizzy” as a universal term to describe feeling faint, lightheaded, or a spinning sensation (either themselves or the world around them). This latter sensation is called vertigo, from the Latin vertere meaning “to turn.”
The most common cause of vertigo is benign paroxysmal positional vertigo or BPPV. Benign means the condition is not dangerous, paroxysmal indicates it occurs in a recurring pattern, and positional refers to the vertigo typically being brought on by changes in position.
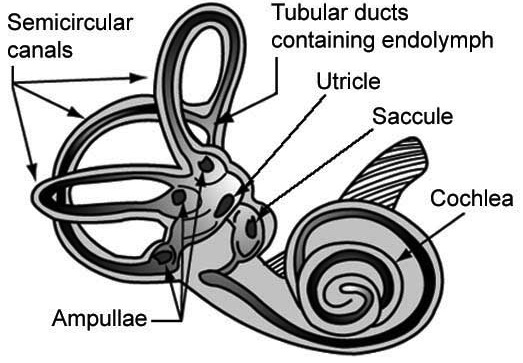
I have to crack open the anatomy and physiology books to explain the cause of BPPV. Hopefully, some of you recall the vestibular apparatus from junior high science class. It is the organ that allows us to maintain our balance and is found in the inner ear. This is a truly remarkable and complex organ. I’ve included a diagram to help you visualize what I’m describing.
We have a vestibular apparatuses on each side of our heads. These organs, along with input from our eyes, are constantly monitoring the position of our heads in space in relation to motion and gravity. If one or both of them gives faulty or conflicting information to our brains, we can lose our sense of orientation in space.
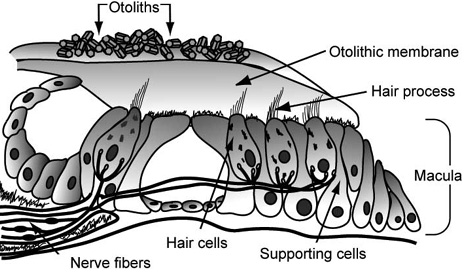
The three semicircular canals are a key part of the vestibular apparatus and are oriented at 90 degree angles to one other. They are filled with a fluid called endolymph. When we move our heads, the fluid shifts to varying degrees inside each of the three canals, allowing us to detect motion in three different planes (head turning, nodding up-and-down, and moving forward or backward). Movement of the endolymph acts on a piece of tissue called the otolithic membrane that resides in two other parts of the vestibular system called the utricle and saccule.
The membrane sits on top of tiny hairs protruding from nerve cells that communicate with the brain. When the membrane moves, it wiggles the hair cells that in turn fire off nerve impulses, telling the brain which direction the head is moving.
Resting on top of the otolithic membrane are tiny crystals made of calcium called otoliths. These crystals provide some weight on top of the membrane allowing it to stimulate the nerve cells more easily.
Now that you’re an expert in some inner ear anatomy and physiology, what does any of that have to do with BPPV? The cause of BPPV is a problem with the otoliths – they get dislodged from their position on top of the otolithic membrane and move into the semicircular canals. The displaced crystals move in the canals tricking your brain into thinking your head is moving. This results in the sensation of vertigo. Tilting the head, rolling over in bed, getting out of a bed or chair, looking up or down, or sudden head motion can all cause vertigo associated with BPPV.
A good patient history is usually suggestive of BPPV. There is also a simple movement test called the Dix-Hallpike maneuver that can be performed in the office to determine if one of the vestibular canals is at fault. You can see a video demonstration here: goo.gl/HCnIDY.
Most cases of BPPV resolve on their own when the otoliths move out of the semicircular canal. Sometimes medications like meclizine (Antivert®) or scopolamine are given to dull the severity of the vertigo.
For those cases of BPPV that don’t resolve on their own, most can be treated in the office by undergoing either the Epley, Lempert, or deep head-hanging maneuvers. These involve putting the patient through a series of movements that attempt to move the otolith(s) out of the semicircular canals. Severe and refractory cases of BPPV occasionally require surgical correction.
{kind=link}