
Blog
My Finger Is Stuck!
By: John Roberts
I have seen many patients over the years who presented with problems getting their fingers to move. They all described pain with “catching” or “popping” when trying to flex or extend a finger. They suffered from trigger finger, a condition also known as trigger digit, or by the medical term stenosing tenovaginitis.
The condition is very common. It is seen two to six times more frequently in women than men and typically presents around 55 to 60 years of age, usually in a person’s dominant hand. It can affect any of the fingers, most commonly in the thumb, followed by the ring, middle, little and index fingers.
The reasons for developing trigger finger are not completely understood. It seems to be associated with activities that require pressure on the palm during powerful gripping or repetitive forceful flexion of the fingers such as when using heavy shears. Unlike carpal tunnel syndrome, the increased use of keyboards in our society does not seem to be a significant factor trigger finger.
Other medical conditions increase the risk of developing trigger finger. It is more common in those with rheumatoid arthritis and diabetes. Those with psoriatic arthritis, amyloidosis, hypothyroidism and sarcoidosis are also at higher risk.
The symptoms and signs of trigger finger are easy to spot. Patients experience the catching or popping sensation when flexing or extending one or more of their fingers. Some may even experience locking of the finger, usually in the flexed (finger down) position. Most patients also have pain in the palm near the base of the involved finger.
Trigger finger is easy to understand looking at the anatomy of the hand that is involved with moving the fingers. Finger movement happens when muscles in the palm side of the forearm contract, pulling on the finger bones. The muscles are attached to the bones by tendons.
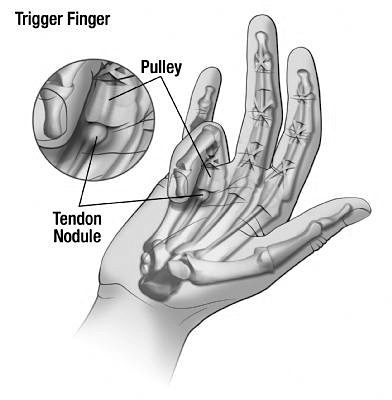
The culprit in trigger finger is one of the flexor tendons on the palm side of the hand, the flexor digitorum superficialis or FDS. In order for these tendons to work properly they have to slide through connective tissue tubes called tendon sheaths and under little tissue bridges called retinacular pulleys. To visualize this, think of a rope that is running through a pulley to pull on an object on the other side.
The anatomic problem that occurs in trigger finger is caused by the development of a swollen area on the FDS tendon. Returning to my rope and pulley analogy, this would be equivalent to having a knot in the rope that can’t pass through the pulley so it gets stuck.
If it’s a small knot, with a little force you can go ahead and pull it through. A larger knot can’t pass through the pulley. This is exactly what happens in trigger finger – as the swelling on the tendon gets larger, it becomes harder to move it through the retinacular pulley and sometimes it can become permanently stuck on one side.
If the enlargement in the tendon gets stuck on the wrist side of the retinacular pulley, the finger can’t be extended and gets stuck in the flexed, or down position. If it gets stuck on the palm side, the finger gets stuck in the extended, or up position and can’t be flexed.
Treatment for trigger finger is fairly straightforward. First line therapy is to try and shrink the swelling in the tendon by injecting a steroid solution into the tendon sheath surrounding the FDS tendon. This procedure can be performed in many physician’s offices using a small needle.
Steroid injections are successful about 85 percent of the time. They are more successful in women, those who have had symptoms less than four months, and who have a single swollen area in the tendon. It is less successful in those who have other conditions such as rheumatoid arthritis and diabetes.
Sometimes a second injection is needed. If a person fails two injections, surgery is usually indicated. It is a simple outpatient procedure that involves cutting the retinacular pulley to allow the tendon to move freely.
– Dr. John Roberts is a retired member of the Franciscan Physician Network specializing in Family Medicine.
{kind=link}