
Blog
Shoulder Pain Part 2
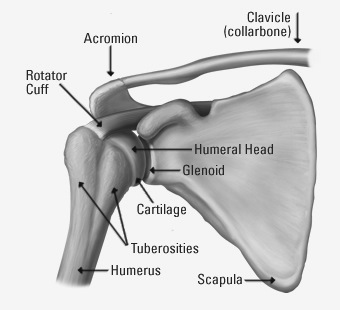
A diagram of the skeletal structure of the shoulder.

Welcome back to my two-part series on shoulder pain. First, I want to do a quick review of shoulder anatomy (see the diagram the right shoulder looking from the front). The upper arm bone (humerus) joins to the scapula at the glenoid and is held in place by two structures: (1) a rim of cartilage (glenoid labrum) that forms a shallow cup for the head of the humerus to sit in, and (2) the rotator cuff which is made up of four tendons that wrap around the head of the humerus.
As I stated last week, in order for the shoulder to move in so many directions, it has to be inherently unstable. Since it is so unstable, two of the most common injuries are dislocations and subluxations. Dislocations result when the ball on the head of the humerus slips out of the glenoid “cup” and remains there. This usually happens when a nperson’s upper arm is hit from behind when the arm is raised to the side and the shoulder is cocked and ready to throw.
A subluxation is less severe than a dislocation. The ball does not completely come out of the cup. Subluxations are usually brief events and the ball returns to its normal position spontaneously but can feel unstable afterward. Dislocations sometimes reduce spontaneously, but often require manipulation by a doctor to get the head of the humerus back in position.
When a dislocation occurs, it can damage structures in the shoulder. The connective tissue capsule around the joint can be torn. One or more tendons in either the rotator cuff or attached to other muscles may be stretched or torn. The glenoid labrum may be torn as well. When these structures are disrupted, it makes the shoulder even more unstable and more likely to cause additional damage and repeat dislocations.
Treatment for dislocations usually involves rest, bracing, and strengthening the shoulder muscles with physical therapy. Surgery may also be required to repair a torn labrum or tendons.
Another very common cause of shoulder pain is bursitis. Most of our joints are surrounded by fluid-filled sacs that pad the structures around the joint, particularly tendons. These sacs are called bursae (singular bursa). Bursae can become irritated, inflamed, and sometimes infected. Irritation of the bursae in the shoulder can occur following repetitive motion of the shoulder. This is commonly referred to as an “overuse injury.” I see this frequently in weekend warriors; not just the folks participating in throwing sports, but also those participating in other repetitive arm motions, like painting their house, trimming trees, or shoveling snow.
Treatment of bursitis can be difficult. Standard treatment consists of rest and antiinflammatory medication as well as icing. Doctors usually recommend non-steroidal medications (NSAIDs) such as ibuprofen (Advil Motrin) or naproxen (Aleve). If those conservative treatments fail, we may recommend more potent steroids, either taken orally or injected into the bursa.
The final cause of shoulder pain I want to discuss is impingement. This term refers to structures in the shoulder coming into contact with one another resulting in pain. Impingement can be bone-on-bone or bone pinching or rubbing a tendon or bursa. While this occurs more commonly in people who have suffered shoulder injuries, it canalso occur in an uninjured shoulder where anatomic structures are naturally close together.
Tendons that have been injured can swell, making them more likely to be pinched or rubbed with shoulder movements. The bones in the shoulder may also develop arthritis with bony overgrowth as a result of injury or natural aging. These overgrowths can lead to impingement as well.
Treatment of impingement varies based on the structures involved. Swollen, inflamed tendons or bursae are treated like bursitis. Occasionally, surgery is necessary to make more room for the structure(s) being rubbed or pinched. This can usually be done through small incisions using an arthroscope.
As always, prevention is the best medicine. If you are involved in sports or work activities that involve a lot of shoulder motion, get involved in a fitness plan to keep your shoulder muscles strong, particularly your rotator cuff. Exercise programs are readily available on the Internet by searching for “shoulder exercises,” or “rotator cuff exercises.” You can find an excellent resource from the American Academy of Orthopedic Surgeons here: bit.ly/3xMPBz
– Dr. John Roberts is a member of the Franciscan Physician Network specializing in Family Medicine.
{kind=link}